

What if two people had nearly identical sleep studies,but entirely different sleep problems? In this episode of Sleep Reimagined, host Nyree Penn dives into the breakthrough concept of neurorestorative sleep endotypes, a new way of understanding why so many struggle to feel restored, even when their sleep looks normal on paper. You'll hear how traditional sleep medicine often misses the root cause of sleep issues by focusing on surface-level symptoms, and discover why sleep is more than just one system—it's a complex interplay of neurobiological processes that can break down in very different ways.
Join Nyree as she break sdown the science behind endotypes vs. phenotypes, introduce the major types of sleep dysfunctions uncovered by this new approach, and share real-world examples of how stress, hormones, circadian rhythms, and even COVID-19 can disrupt your most fundamental need: restorative sleep. If you've ever felt frustrated by ongoing fatigue or brain fog, despite doing everything "right," this episode is for you. Discover how uncovering your unique endotype could be the missing link to truly feeling restored.
00:00 Understanding insomnia and endotypes
06:06 Understanding sleep challenges and solutions
07:07 Identifying complex sleep issues
11:31 Understanding Hyperarousal and Sleep Issues
14:21 Addressing sleep and hyperarousal issues
18:51 External sleep disruptions and menopause
22:14 Understanding restorative sleep loss
23:30 Treating chronic insomnia patients
28:47 Optimizing employee work schedules
31:16 Importance of sleep and products
35:34 Testosterone shots and sleep issues
37:23 Importance of Deep REM Sleep
43:08 Understanding sleep endotypes
44:22 Introducing insomnia sleep innovation
48:04 Virtual sleep services overview
51:21 Introducing the sleep apnea pillow
54:26 Understanding sleep problems and solutions
Sleep Isn’t One-Size-Fits-All: Insights from “Sleep Reimagined” with Neurorestorative Sleep Endotypes
What if your sleep study looked perfectly normal, but you still woke up every morning feeling exhausted, foggy, or unrestored? That’s the provocative question at the heart of the first episode of “Sleep Reimagined,” where Nyree Penn peels back the layers of traditional sleep medicine to introduce a groundbreaking new lens: neurorestorative sleep endotypes.
In most clinics, a typical approach to sleep problems revolves around what’s visible on a polysomnography (PSG) sleep study. If you’re diagnosed with sleep apnea, a CPAP machine is likely prescribed. If there’s no obvious breathing or moving issue, medications are the next step. But, as Nyree Penn points out, there are “hundreds of thousands” of people whose sleep studies look normal, yet they can’t find relief from persistent sleep problems.
Sleep Is More Than Meets the Eye
The episode starts with a simple car analogy: two identical Teslas might both have their “check engine” lights on, but the underlying problems could be radically different under the hood. This, Nyree Penn explains, is the core difference between phenotypes (what a problem looks like on the outside) and endotypes (the deeper reason for the issue). With sleep, you may look tired, but the cause can be stress, pain, hormones, or something more neurological.
Traditional sleep medicine focuses mostly on phenotypes and Nyree Penn believes that’s left a critical gap, especially for people whose suffering doesn’t fit into neat, textbook categories.
Enter Neurorestorative Sleep Endotypes
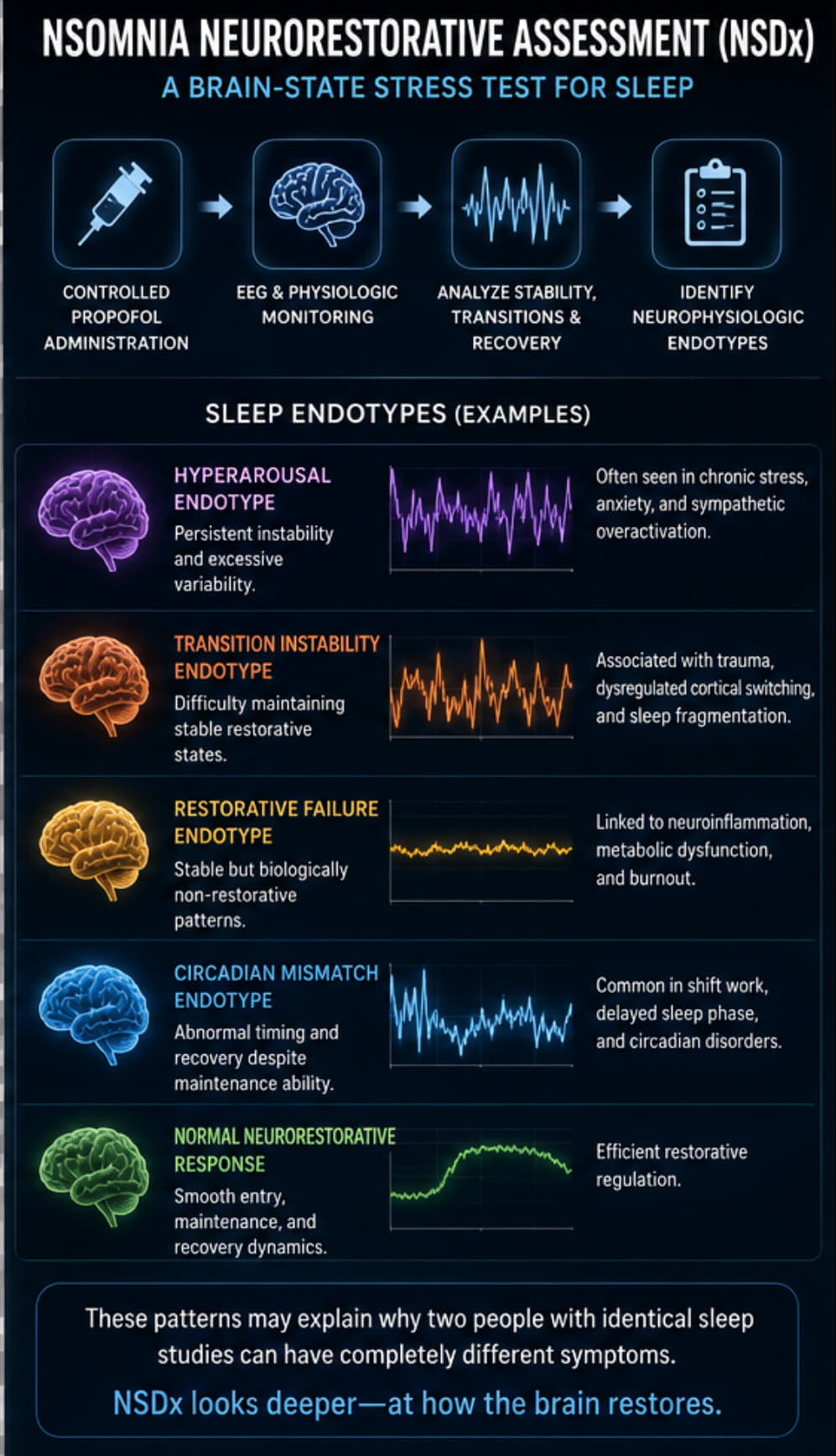
The discussion introduces “neurorestorative sleep endotypes,” a new classification system that gets to the root cause of non-restorative sleep. Instead of focusing solely on sleep breathing or movements, this system considers the neurobiological processes needed for truly restorative rest. Nyree Penn details five main endotypes identified in her practice:
Normal Sleep
Hyperarousal Endotype – typified by the “wired and tired” feeling, and often seen in people with backgrounds in high-stress, anxious environments.
Transition Instability Endotype – trouble staying asleep, often due to pain, hormonal shifts (like menopause), or environmental disruptions.
Restorative Failure Endotype – people who sleep through the night but still wake up exhausted. Sometimes, this involves long-term neurological changes, potentially even post-COVID.
Circadian Mismatch Endotype – when internal clocks and schedules are out of sync, as in shift workers or extreme night owls.
Why Does This Matter?
“Same sleep study, different brains, completely different outcomes.” That phrase isn’t just a catchy slogan, it’s a window into why so many people have been failed by simplistic sleep frameworks. The real breakthrough is acknowledging that neurological processes like adenosine (sleep pressure), GABA (calmness), and dopamine (motivation) all play roles in how and whether we truly restore during sleep. A normal amount of time spent in bed doesn’t guarantee actual restoration.
Importantly, the episode highlights how poorly matched treatments (prescribing a CPAP to someone without sleep apnea, or medication for someone with a deeper neurobiological problem) can leave patients feeling lost and frustrated. Recognizing your unique sleep endotype could be the key to retraining your brain and finally experiencing restorative sleep.
Hope on the Horizon
The NSDX assessment (NSOMNIA Diagnostic Neurorestorative Assessment) offered by Nyree Penn’s team marks an innovative step, utilizing medical anesthesia and in-depth neurophysiological monitoring to pinpoint exactly which part of the sleep “engine” isn’t working. This unlocks the path toward individualized therapies to restore natural, healthy sleep often going far beyond what medication or basic sleep hygiene alone can provide.
Their message is clear: Sleep isn’t a one-size-fits-all process. By looking deeper past what’s merely visible on the surface, there’s real hope for even the most baffled insomniacs.
Key Takeaway:
"The goal isn’t just more sleep. It’s restored sleep.” If you’re struggling to feel rested no matter what you try, the emerging science of neurorestorative sleep endotypes might finally offer you answers and lasting relief.
Show Website - https://sleepreimaginedshow.com/
Nyree's Book - Why we don't sleep
Nyree Penn's LinkedIn - https://www.linkedin.com/in/nyreepenn/
NSOMNIA Sleep
@NSOMNIAsleep
TopHealth Media Website - https://tophealth.care/
“Disclaimer: Informational only. Not medical advice. Consult your doctor for guidance.”
[00:00:00] So for instance, we see a million white Teslas everywhere. But your Tesla may have a different problem than my Tesla. So even though they look the same on the outside, their phenotype looks the same. If your check engine light is on, it may be a different issue, a different endotype. And that's how we describe what people are experiencing when they experience insomnia. Most of our patients come in and they say, oh I'm sleepy, I can't sleep. And then naturally I'm like, okay, but why?
[00:00:29] But it's because, oh, because I'm a new parent. Or because I'm so stressed out at work. Or because I just lost a parent. You know, those are different endotypes. So that's saying your physical appearance is sleepy. But your underlying endotype is different. And that's what we look at in some new sleep.
[00:00:47] What if two people had nearly identical sleep studies but completely different sleep problems? That's the gap we've been missing in sleep medicine. Because sleep isn't one system.
[00:01:14] It's a set of neurobiological processes that can break down in very different ways. So today we're introducing a new framework, Neuro Restorative Sleep Endotypes. A way of understanding why people don't feel restored even when their sleep looks normal on paper. So I'm excited to have this conversation with you, Nairi. It's always great to see you. How are you today? I'm good. How are you? Hello. Good, good. We talked a little bit about this last time.
[00:01:38] So I'm excited to kind of dive in and maybe even go back to basics a little bit to really understand what endotypes are and really hop into the science behind it. Absolutely. Layla, thank you so much for taking this time to speak to us at Insomnia about the difference between an endotype and a phenotype. And I know these are very scientific words that people may or may not have heard before.
[00:02:00] But these are terms that we use at Insomnia to identify what people's sleep disorders are and where they fall into a category. So, for instance, let's say you have a car, right? And you can have a Tesla, for instance, and we see a million white Teslas everywhere. You want to call me because I know you need some sleep. But, you know, your Tesla may have a different problem than my Tesla.
[00:02:25] So even though they look the same on the outside, their phenotype looks the same. Their physical appearance of a white Tesla looks the same. If your check engine light is on, it may be a different issue, a different endotype. And that's how we describe like what people are experiencing when they experience insomnia. So a lot of people say, oh, I can't sleep. Okay, that's great. But what does that mean? Why can't you sleep? And that's the endotype.
[00:02:55] And that's what we identified Insomnia Sleep. We identify your sleep endotype. Most of our patients come in and they say, oh, I'm sleepy. I can't sleep. And then naturally I'm like, okay, but why? You know, it's because, oh, because I'm a new parent or because I'm so stressed out at work or because I just lost a parent. You know, those are different endotypes. But your physical appearance when you come to me is that you can't sleep. So that's the difference between an endotype and a phenotype.
[00:03:24] So that's saying your physical appearance is sleepy, but your underlying endotype is different. And that's what we look at at Insomnia Sleep. As a society, we've done a great job of telling people they can't sleep. And unfortunately, right now, prior to Insomnia Sleep, the only other option was, okay, I can't sleep. My phenotype is I can't sleep. Let me go get a sleep study. Right?
[00:03:47] Your doctor will tell you go get a sleep study, you know, spend the night, get a PSG, a polysomnography, which also starts with a P. And they tell you your phenotype. They tell you if you stop breathing. They tell if you're moving. They tell you if you're clenching. They don't tell you what your endotype is. Why can't you stop moving? Why do you snore? We do that at Insomnia Sleep. And so we identify your endotype. Got it.
[00:04:15] And so you introduced a concept called Neuro Restorative Sleep Endotypes. But now that you talked a little bit about what an endotype is, why is this potentially a major shift in how we think about sleep problems? Prior to Insomnia Sleep, nobody was looking at sleep from a neuro restorative perspective. We can go to sleep and put our bodies down. We can sedate, but we don't necessarily restorate. That's what we do in Insomnia. We look at sleep from a neurological perspective.
[00:04:42] So this is so important because now we're advancing sleep medicine. We're going past sleep apnea. We're going past movement disorders. Now we're looking at the brain. What is your brain doing? Can you restore? Can you stay asleep? Do you have the neurophysiology to wake up, restore and transition and get restorative sleep? And that's how we're different. And that's what we look at in Insomnia Sleep.
[00:05:07] And you shared a chart with us that we'll make sure to include in the show and make accessible for everyone to see as well. But on that chart, it says same sleep study, different brains, completely different outcomes. Absolutely. And that sounds like such a really well-worded phrase, but why is that such an important idea? That goes along with the importance of advancing sleep medicine.
[00:05:33] Unfortunately, right now, the only other options are CPAP machine if you have sleep apnea or medication. You know, there's so many, there's hundreds of thousands of people out there who don't have sleep apnea. Absolutely, sleep apnea is important. Absolutely, PSGs identify whether or not you have a sleep disorder during your sleep. Do you lose oxygenation? Do you stop breathing? But what if you don't? What if you don't have sleep apnea and you still can't, not just sleep rest.
[00:06:02] My brain won't turn off. Brain fog. I'm constantly thinking, I put my body in, but my eyes are wide awake. There's only so many sheep I can count. This is what we look at in Insomnia Sleep. What is going on neurologically? So when we identify endotypes, your sleep endotype, we tell you why you can't sleep. Okay, we do identify, we do absolutely identify if you have sleep apnea. But if you don't have sleep apnea, then you have to come in for a neuro restorative sleep assessment. We'll identify your different endotype.
[00:06:32] We've identified five essentially at Insomnia Sleep. Those five are naturally a normal sleep. Can you go to sleep and restore? Do you have hyper arousal syndrome? Are you too stressed out? Do you not know how to relax? You bring your problems to bed with you. And just because you lay your body down, your mind is still going. Are you on certain medications that are preventing you from sleeping? Does pain or menopause cause you from not sleeping? There's so many reasons why people aren't sleeping. It's not just sleep apnea.
[00:07:02] So unfortunately, prior to Insomnia, the only other options were CPAP machine, sleep apnea, or medication. But what if you don't want to take medication? You have to come to Insomnia Sleep and get a neuro restorative sleep assessment so we can actually identify why you're not sleeping. And then with that, two people can have identical sleep studies, right? But why would they have exactly the same sleep studies but actually completely different neurological sleep patterns? It comes back down to the PSG.
[00:07:32] Like I said, as of right now, polysomnography prior to Insomnia Sleep was the only way to identify if people had a sleep problem. However, it's important to identify and recognize that PSGs only identify if you have a breathing problem or a moving problem. They do not identify if you have a neurological issue or concern. And that's what we do at Insomnia Sleep because we are the first of its kind.
[00:07:58] We identify that sleep is just more than if you stop breathing, if you stop moving. What if you are stressed out? What if you have menopause? What if you have pain? What if you don't have the ability? You know, just as of recently, I read an article where they're saying that COVID may be disrupting people's neurology based on the receptors that were affected by COVID. So I'm starting to have a lot of patients who experienced COVID and now can't sleep.
[00:08:27] There's something there, you know, and that's neurological. We look at sleep from a neurological perspective, not sedation, restoration. Absolutely. That's interesting because since COVID was about six years ago now, I feel like we're going to probably start to see all these effects that are more long-term effects. That's interesting. All the effects, you know, everything, you know, people said, because we didn't know. Like we didn't even know about COVID until it happened. So naturally, now we're starting to identify things.
[00:08:55] For us at Insomnia, we're identifying sleep issues and chronic neurological sleep issues, not just, oh, I can't sleep anymore. It's like, I cannot turn my brain off. There's a restoration issue there. And we look at sleep from a restoration perspective, not just if you can close your eyes. Can you restore? Can your brain do what it's supposed to do during deep restorative rest? Absolutely. And so one of the endotypes you mentioned was hypoarousal endotype.
[00:09:25] So what does that look like in real life? And why do you think that so many people just describe themselves like we've talked about before as wired and tired? Absolutely. That's one of our most recognizable endotypes is hyperarousal endotype. How that presents to us is wired and tired, right? Those are those people who are always anxious. You know, those people, they make you anxious for no reason, right? They're just always on go, go. And you're just like, hey, bro, I don't know what's going on. But if you could just calm down, take it down a notch. They're always like that.
[00:09:55] They're hyperarousal state. They live there, right? So imagine what their sleep looks like. It's their list. They're off the chain there. But this is them naturally. It's a problem when it affects their sleep. So in those people, they're already at a hyper vigilant state naturally, right? High acetylcholine, high cortisol, high adenosine, high everything, right? They're always on go. However, when it's time for them to go to sleep, they also don't know how to turn it off.
[00:10:23] So in those hyperarousal states, how that presents to us at insomnia sleep is I'm always going, I'm always wired, but I'm never restored. They don't know how to rest. Their brains don't know how to convert and restore and rejuvenate because it just hasn't had the ability because internally there's something going on inside their brains where adenosine, adrenaline, all those are always on high.
[00:10:49] So for their sympathetic, for the dopamine and all those feel good and let's calm down in the gabbers to take effect for us to rest. It's a little bit more challenging for them. And so from an anesthetic perspective and an insomnia sleep, for us, those people present is we have to use more anesthesia to calm them down. Right. Which makes sense. Over the counter medications haven't been helping.
[00:11:13] You know, meditation is absolutely one of our therapies that we recommend for those type of people to help their brains learn how to calm down. And it's just a habit. You know, depending on your upbringing, a lot of people were raised in hyper vigilant households. This is all they know. Their parents were this way. Their grandparents are this way. Their aunts and uncles are because their whole family is this way. So to them that's normal. Right. But it's not normal to not be able to let your mind rest.
[00:11:41] So we help them find coping mechanisms to help them down regulate and be able to just not be so hyper aroused because that's internal. There's nothing we can do about that internally. I can give you medication to make you, you know, suppress it. We use the anesthesia to get you to calm down, to get you that restorative rest. But when you go home after your neuro restorative assessment, what are we going to do? We give you our therapy, the insomnia sleep assessment for hyper arousal.
[00:12:11] And that's how we treat our patients who are in that state. So we'll identify it, but we also help you identify therapy mechanisms. And meditation is absolutely one of them. That's so interesting. I didn't realize that that was a part of it as well, because like you mentioned, people that have that upbringing and things like that hyper arousal state probably becomes like their baseline of normalcy. They're ready to go. Always, always. Right.
[00:12:36] And for us, for surgical procedures, I have to give them more anesthesia because their body is naturally up. Right. So they take more anesthesia than the average person would. Not their fault. That's just how they're wired. But it's important to again, identify you can't sleep. But why? Because you have hyper arousal syndrome. Right. We dig. We give you therapy. Why are you always stressed? Is this how you were brought up? Is there something going on? Do you feel like you need to catch up? Did something happen?
[00:13:06] We're the only company who really looks at and takes the time to help people with their sleep disparities. Sleep affects every aspect of everyone's life. But what is it doing neurologically? There's only so much drugs you can use. We got to figure out the root cause and the problem. And that's what we do in insomnia sleep. Absolutely. And so, for example, when someone says to you or comes to you and is saying, you know, my brain just won't shut off. Is that what they're really describing from like a more clinical perspective? Is it hyper arousal endotype?
[00:13:36] Yes, absolutely. There's actually people out there with normal sleep. And that's actually another good point. Side note. But we take sleep for granted. Before I started the sleep company, I did not have a sleep problem. And I'm very, very grateful to say I can sleep. And now that I recognize, you know, whatever's going on, I have sleep issues once in a while. But on a chronic, constant, consistent basis, no. And so we take sleep for granted.
[00:14:01] You know, it's the most frustrating thing when you lay down at night and you can't close your, you can't let your brain rest. Right? And for them, they're very frustrated. We have a lot of frustrated people who can't sleep. Understandably so. Especially when you did everything you were supposed to do. You got a PSG. They said you don't have sleep apnea. You don't want to take any more medication. The melatonin is not working anymore. And what you said, too, is you don't have chronic sleep problems. But once in a while, I'm the same way.
[00:14:30] I think, you know, luckily I'm not, you know, someone who has chronic sleep problems. But those times that I can fall asleep are so frustrating. I mean, like, so, so frustrating. And it's just like, the more you try to fall asleep, the more you're thinking about going, Everybody should be able to sleep. Why can't I go to sleep? And that's the thing, too. Like, it's such a personal, intimate thing. Your rest. We don't talk about your inability to not sleep, but rest. I'm not minimizing, you know, our body. There's two sleeps. I've said this multiple times.
[00:14:59] There's your body sleep and your mind sleep. We focus on your mind sleep, your brain sleep. So absolutely, when people say my brain won't turn off, that's absolutely those people we want to help. And then another endotype is transition instability endotype. So what is that? And why do you think that some people seem to be unable to stay asleep, even if they do fall asleep early?
[00:15:23] When we refer to transition instability, that's the people that we see who tend to, which is so crazily ironic. But those are the people we see that are taking sleep medications, but they're not resting. Right. So their inability to transition into restorative sleep has been blocked or hindered in some way. Another example of that is pain. Right.
[00:15:49] People are in chronic pain, neuropathy, diabetic neuropathy, stroke neuropathy, injury related neuropathies. Those type of pain signals will wake us up out of our sleep if it's chronic. We can be in deep sleep and all of a sudden we're in pain. Right. So that fragments our sleep. So now our brains are like, I'm so sleepy because I'm in pain. Another example of that is menopause and it's not specifically menopause.
[00:16:14] It's the hot flashes associated with menopause that wake us up out of our sleep, which cause us to have the inability to get restorative sleep due to the fragmented hot flashes we have throughout the night. So that's the idea behind. So you have the ability to sleep.
[00:16:32] It's just some sort of external pain, neuropathies, hot flashes, bed partners, pets, children, TVs, air conditionings, you name it, neighbors. It's some sort of external event that prevents us from getting that restorative sleep or fragments it. So that's the transition instability.
[00:16:53] And one of the most fascinating categories is the restorative failure endotype because it might be similarly confused with another one, but this is different than all other endotypes. So how is it possible that someone can really sleep through the entire night, but still feeling exhausted when they wake up? This is probably one of the most misunderstood phenotypes. So the restorative failure, and I don't want to make it so dismal.
[00:17:21] However, the restorative failure endotypes that we've identified is that what happens is these people actually have lost the physiological ability to get into restorative sleep. Remember something we also focus on is are you restoring? It's fine. You go to sleep. It's fine. You get your brain rest, but are you restoring? Are you getting the restorative benefits of neurological deep restorative REM sleep? These people cannot.
[00:17:49] These people are actually fall into the category of our COVID patients that we've we've seen recently to where there seems to be something that the COVID virus has either affected their GABA B specific receptors. I don't want I don't mean to get too sciencey on you, but this is what happens with restorative failure. These people go into the cycles. They sleep six, eight, ten, twelve hours of sleep. However, when they wake up, they do not feel restored.
[00:18:19] They're still just as miserable as they were before. They still experience brain fog. They still have psychological issues. They still have physical issues. They still feel like they're not getting that restorative sleep that their brain so desperately needs. And we've been able to identify that these people are in restorative failure. These are our restorative failure endotype patients. And these are definitely our chronic insomnia patients who've lost the ability to get into restorative sleep.
[00:18:48] So our therapy for them is very, very invasive. Invasive in the sense of we do definitely have two week therapy with them as opposed to one month therapy with them. Their therapy sessions tend to be longer because it's more chronic and it's more embedded physiologically. So we do offer therapy for these type of patients, all of our endotype patients, but they're very specific based on their endotype. And so that's the importance of having the diagnostic assessment first.
[00:19:16] So we can identify your specific endotype. And then so is the restorative endotype the reason that so many people have a normal sleep study, but they still really struggle with the fatigue and the brain fog? Absolutely. And this is definitely the foundation behind insomnia sleep. Even if you don't have to have sleep apnea to have sleep problems, you don't have to have take medication to be able to go to sleep. This is a biological necessity.
[00:19:45] Why do people feel like they need medication to reach that? They don't. There's we're solving the symptoms, right? As a society, we've identified the phenotype. You physically look like you're tired. You know, you've seen those people. Girl, what's going on with you? You look so tired. What's going on? Oh, this, that, this is what's going on. You know, my life. Okay. Granted, that's, that's legitimate. Right. But you don't have sleep apnea. You don't need a CPAP machine. You don't want to get on medication.
[00:20:13] You're tired of taking melatonin. You've tried alcohol. You've tried THC, but you're not restoring. And that's why they've done everything you're supposed to do. You've gotten your PSG. I've talked to my doctor. I don't have sleep apnea because you have a neurological issue. There's a root cause. What or why are you not sleeping? And that's what we look at at insomnia sleep. We're not identifying phenotypes. We identify endotypes.
[00:20:42] What's going on in your brain neurologically that you can't rest. So another endotype that I want to talk about that I think is super interesting is the circadian mismatch endotypes. How is it different from someone who's simply a night owl or thinks of themselves as a night owl? So, you know, you said thinks that they're a night owl. If I can give the audience any information right now is to figure out what your own sleep requirements are and when.
[00:21:10] So how long and how much some people don't have no idea how much sleep they need or want. And I say sleep because it's relative, right? Some people need six. Some people need four. My dad only needed four hours of sleep and he functioned just fine. Some people need 10 hours growing teenagers absolutely need 10 to 12 hours. Parents let them sleep these teenagers, especially the boys. They need the sleep girls during their periods. They need to sleep. Let them do that. All right.
[00:21:39] And it doesn't necessarily have to be on your schedule, but at least allow them the opportunity to just rest. So knowing it is so important for us to know how much sleep we need and when. Right. Like you said a night owl. My brother, he is a night owl. He does not shine before 10 p.m. But that's his thing. Okay. Just know your vibe. Know when you perform your best. And that no one's ever asked you, oh, when do you like to sleep?
[00:22:08] How much sleep do you need? Every person that comes to work for insomnia, we ask that question. If I have an employee who performs better at 3 p.m., I need to consider that. They probably need to be on the 3 to 11 shift. Right. So that's important. Even as an employer, know when your employees do best. Schedule your meetings around that time because you know everyone. Try to find a window. Maybe it's 12.
[00:22:35] Your morning larks who like to be there at 7 a.m. until 3, you know, a 10, 12 window of a meeting is great. And so those are just things to keep in mind. Being a night owl actually means something. A morning lark means something. When do you perform your best? So that's what we look at with our circadian mismatch patients. That is legitimately a question we ask them. When do you perform your best? We give them a sleep test that helps them identify their sleep character.
[00:23:04] A morning lark. A night owl. Now there's different animals associated with these preferred hours. But if we have a night shift worker, you're not going to stop working at night. But you know during the day when everybody else is awake, you're mismatched, right? The sun is up, but you need to be asleep. And what happens is through time chronically, your brain is doing exactly what it's supposed to do.
[00:23:29] It's just you haven't established the habit of getting it into that system to where it can reestablish that neuroplasticity. And it knows when it can rest. You just need to tell your brain when you can rest. Granted, ideally sleeping according to the sun is best because we are creatures of this earth. Something about dogs, fun fact. They sleep according to the sun. When the sun goes down, no matter where you are, when the sun goes down, your pup is asleep. Okay?
[00:23:58] Especially if they're puppies, they need more sleep because they're animals just like we are of this planet that follows the sun. Circadian is so important. We absolutely look at the wearable devices of these patients. You know, if you are a night shift worker and you're up and you need to be more alert, we just get you into the habit of having a consistent day schedule. Just, it's a habit. Get your brain into the habit of knowing when it can go to sleep.
[00:24:26] We don't rest if we don't feel safe. And that's a physiological requirement. We have to, so if you know, you got to pick up the kids at three because you work the night shift, because your family, your significant other works during the day, and you work at night because you have a family and children responsibilities, and you need to be up at three. You know, your window is whatever, you know, seven to 11, whatever, however you want to work that out. But do it. It's a pattern.
[00:24:55] The blackout curtains, so important. We're huge advocates of sleep masks. Go to our website, insomniysleep.com. We have sleep masks. We have sleep masks we prefer to use. We're big on blocking out the light. That's what's so important with our patients with circadian mismatch. You just got to get them to align with what their work schedule is. That's so interesting. I never knew that existed because you always, I mean, I've heard people, I'm more focused at night.
[00:25:24] So it was always something that I would think of as, like we said, like a night owl. You just, you know, creature of the night, prefer the night. But to know that there's actually reasoning behind that is so interesting. Absolutely. And so we talked about how, you know, hormones and work and all of these things can contribute to different sleep patterns. Right. So do hormones and shift work and parenting and menopause and, you know, all these modern lifestyles contribute to circadian mismatch? Absolutely.
[00:25:53] Not so much circadian mismatch. You know, everybody has different reasonings. Like I had mentioned with circadian mismatch, we see that a lot with our night shift workers or people who have inconsistencies. So that's something else I want to bring to your attention too. There's a lot of jobs, military, hospital, police, fire, you know, our community workers. We have these odd shifts, right? And not so much odd shifts.
[00:26:20] It's odd shifts to where they're extremely like to a 12 hour difference odd shifts. We might be on call one day, you have a day off and then you're back to the day shift. You have a day off and then you're back to the night shift. This is very dangerous, right? This actually contributes to long term circadian mismatch damage.
[00:26:40] And this will actually lead to restorative failure endotype because if your body doesn't know and your mind doesn't know when it can rest, your day this time, night this time, it's a very huge problem that we need to start addressing. And I understand people aren't going to quit their jobs because sleep and I get that. However, it's important to have inconsistency because that doesn't necessarily mean that you're a night shift worker.
[00:27:09] It could just mean you're an inconsistent worker. You have a type of shift that requires you to be up during the night and the day. So imagine what your brain feels like when you try to go to sleep on a Thursday, right? And so that's what we work with. There's no amount of medication that can help that. There's not a CPAP machine that can help that. It's neurological. And that's what we do at Insomnius Sleep. We help people identify. We've got to identify what your endotype is.
[00:27:35] Like I said, first with the assessment and then we'll provide a therapy or a treatment. And then when it comes to hormones, like I said, that could be another. That's transition instability. Because with the hormones, it's not menopause. It's the hot flashes associated with menopause that cause you to wake up during the night. So that's hormonal, right? That's important to look at. That's why we measure hormones.
[00:28:01] We do neurotransmitter and hormonal testing for women and men. Same thing with testosterone. That's no different. Testosterone tends to give them more energy. So if they start taking these T shots, all of a sudden they couldn't sleep. And I know doctors recommend that. A lot of the doctors, the male doctors you have and the longevity doctors on the Top Health Channel, they definitely recommend. And we do too. However, it's important to understand that you probably will have some sleep issues at the beginning. Because testosterone actually gives you energy.
[00:28:31] You know, it wakes up our guys. It gives them, it increases. Now they want to work out at night, right? So now it's changed their lifestyles. So now you're hyper, you're up, you're at the gym, you got a T trying to get your gains, that pump on, and then you go home an hour later, take a shower, go to bed. That's what we look at. So hormones absolutely do affect the different endotypes. And we identify, is it the testosterone or is it something more neurophysiology associated with your insomnia?
[00:28:58] Beyond that, where do neurotransmitters really come into this? So for example, you've talked about, you know, dopamine and GABA, glutamine. So how do all of these neurotransmitters fit into these endotypes? At insomnia sleep, one of our core principles is that we identify sleep from a neurological perspective. So we have to go back and identify what does affect sleep and our ability to get restorative sleep neurologically. And that's adenosine.
[00:29:25] Neurotransmitter is our energy building block. That's what gives our brains energy. So during the day, as we use energy, as we move our bodies, as we use our brains, we start using that energy. ATP, adenosine triphosphate. As our brains need more energy, it breaks that down, right? Energy breaks that down. We're working out. We're working. We're, you know, taking care. We're going to school. We're doing it. We're living our lives, right? At the end of the day, when we go to sleep, we need to restore that energy. We need to refresh, rejuvenate.
[00:29:55] And that is what REM sleep, deep restorative REM sleep allows us to do. It only happens, that restorative ATP regeneration only happens during deep restorative REM sleep. However, if we're not getting there, then we're not restoring. So our brains do not have the energy to consider what it needs to do for the next day to recharge, to feel refreshed and rejuvenated. So from a neurologic perspective, the neurotransmitter adenosine is everything.
[00:30:25] That's the foundation to insomnia sleep. And that's the foundation to sleep pressure and homeostatic sleep pressure. That's the second sleep that I always keep on referring to. And if that isn't recharged and rejuvenated, then we have neurological dysfunction. Another neurotransmitter that's very intrinsic to this process is GABA. GABA allows us to calm down. That calming, let us get ready for bed and relax and restore.
[00:30:53] However, like I said, we're a system. It's not just one. We're like a car. One, I don't just need an engine. I don't just need the body. They have to work together. And we have to, there's so many, there's 10 neurotransmitters that affect that. Essentially it's fight or flight, right? We're up or down. Dopamine is another one that's very important. That has to do with mood and motivation. Acetylcholine suppresses all of that. So if you're acetylcholine, cortisol suppresses all of that.
[00:31:22] So it's like a switch that occurs every day. And our neurotransmitters are always in play. Always. But there's five and five. And they counter each other or support each other. And that's what we look at in some of these sleep from a neurological perspective. And we do neurotransmitter testing because in addition to GABA and adenosine, dopamine, glutamate, serotonin is also a huge neurotransmitter that we look at. And so that's why we do a nutrition plan. 80% of our serotonin is made in our gut.
[00:31:52] If we don't look at that and you're still having a sleeping problem, then we're not doing our job. So we look at everything from a neurological perspective. So we absolutely do neurotransmitter testing and hormonal testing when we do your neurorestorative sleep assessment. And then you mentioned adenosine. So can adenosine and sleep pressure be completely normal, but yet still really fail to achieve restorative sleep? That's a really tricky question. So adenosine is what causes the sleep pressure.
[00:32:22] So think of it like almost like a door, right? And when you close the door, you go behind closed doors in your room, you go to sleep, you restore, you rejuvenate, you do all that. But you know, in the day when you wake up, you're restored, you open the door, you go about your day, you come back behind closed doors, that sleep pressure. If you don't open that door and relieve that sleep pressure, your brain doesn't have the ability to have enough energy it needs to go out and do what it needs to throughout the day.
[00:32:52] So for someone to say they're restored or not restored is a big deal. We don't necessarily measure sleep pressure. We measure your ability to have restorative sleep. And we use adenosine to identify that. So they're interrelated in the sense of we use adenosine to determine whether or not you have restorative sleep pressure. How we do it at insomnia sleep is with our insomnia sleep assessment.
[00:33:20] We use propofol to release that adenosine and that's the novelty and the innovation behind what we do at insomnia. We've identified that we can actually use an anesthetic propofol to relieve that adenosine sleep pressure. However, does that mean you're restored, right? Does your brain have the ability? Once I give you propofol, does your brain have the neurochemical and neurophysiological
[00:33:48] ability to get into restorative REM sleep? I'm not sure. And that's what we identify at insomnia sleep with the different endotypes. And then once we identify if you do, we will give you a treatment plan and insomnia sleep therapy to help you reestablish that neuroplasticity to get you restorative REM sleep on your own. So, and then beyond that, how does NSDX help identify a person's narrative sleep endotype?
[00:34:18] So NSDX stands for the insomnia diagnostic neurorestorative assessment, NSDX. When we do the one hour assessment, people come into the clinic, we do the assessment, we use the anesthesia to put you into deep restorative REM sleep. Once we get your brain into the state, so I know you can get into restorative sleep because I use the anesthesia to get you there. But when I turn off my anesthesia, what does your brain do?
[00:34:46] And that's what we look at. So identify, does your brain, do you just immediately wake up because you have hyperarousal endotype? Do you stay asleep because you have restoration failure? Do you wake up and then go back to sleep because you have circadian misalignment? So that's what we identify. We identify which endotype you have. Once we get your brain restored and rejuvenated and relaxed, what does your brain do?
[00:35:15] Because your circuitry will only follow what's wires together, fires together, right? So your brain will only follow what fires together. But what has been firing together is not getting you restorative sleep. And that's what we look at, at insomnia sleep. And we develop your own personalized treatment, your own personalized sleep plan based on your endotype to get you to reestablish that neuroplasticity and that wiring so you can do it on your own.
[00:35:41] And then for someone who is listening right now, what are some of the biggest signs that they may be treating maybe the wrong sleep problem? And why is identifying their endotype so, so important? I want to definitely start out all of this by saying we have, I'm so grateful that insomnia has been able to bring this innovation to the market and offer this to the consumer market, right?
[00:36:06] Medically, anesthetically, if you weren't having some sort of surgical procedure, then we would not have had the ability to offer that. But now with insomnia sleep, we can now really help people from a neurological perspective to help them with their sleep issues. Prior to insomnia, the only other option most people had was a PSG that only identified if you had sleep apnea, if you were moving or sleep medication, right?
[00:36:33] So if you don't have sleep apnea or you don't want to take sleep medication and melatonin is not working anymore and you're tired of drinking and smoking and taking gummies, I'm not knocking that. But let's identify why, because clearly it hasn't been working. So that's what we do at Insomnia Sleep. We identify why your sleep is broken from a neurological perspective. And I don't mean to say broken as if, you know, people are doing anything wrong. It's just when you've run out of options, you for sure start to internalize that.
[00:37:01] Sleep is so intimate and personal. There's so many factors that influence that. As medical professionals, we weren't really taught that. In medical school, it's like, okay, write a prescription, right? We can help them to an extent, send them to go get a sleep apnea test. I don't know. But after that, even as medical providers, we're at a loss for options. And that's what we do at Insomnia Sleep. That's all we do. We just look at people's sleep. I speak to you. We consult you. We coach you. We help you develop your own personalized sleep plan. It's so personalized.
[00:37:31] And I'm so happy to say that I think that's where sleep medicine is going now. Personalized sleep medicine. Because just because you had the same sleep study as your twin, doesn't mean that neurologically you're having the same sleep issue. So that's what we look at Insomnia Sleep. That's why the neuro restorative assessment is so important. So we can identify your endotype and give you the treatment plan that you need to get you the therapy for your neurological Insomnia. Absolutely.
[00:38:00] And I think even something we were chatting about earlier was I was, you know, self-diagnosing and thinking that one of my endotypes would have been the endotype that I have. And through talking to you, I realized that it wasn't even the right one. So it's super important to realize what the correct one is for you, you know, talking to you and talking to an expert so that you can really identify the right one. Because from a non-medical perspective, you might think you're fitting in one category when it's not right.
[00:38:29] And then it's not going to benefit you. You're going to be doing the wrong things because it's not the best applicable thing for you. And, you know, also, I just, I just want to point out too, that I keep on referring like our neuro restorative assessment. Yes. That requires that you come to the clinic. You have anesthesia, you have the anesthesia sleep therapy that we provide. Same thing for our insomnia sleep therapy. It does require that you come to the clinic based on your endotype and you will have the anesthesia sleep.
[00:38:56] However, I do want people to understand that you don't necessarily have to come to the clinic. We have other virtual services that we can offer. I consult with patients. I have a 90 minute consultation that I do. We do a medication management plan. We do a nutrition plan. We identify just like we spoke earlier about you thought you had one issue when actually it was another type of endotype. That's what I do. I spend 90 minutes speaking with our patients virtually. It's over Zoom.
[00:39:23] We can definitely speak to you, identify what other things that we do. We do the assessment. We can send the home sleep test to you, the sleep apnea, all these. We have so many other virtual services just to get you to, let's just get the ball rolling, right? This has not been offered. This is not really offered anywhere else in the world. We are the only company in the world that offers to identify sleep disparities from a neurological perspective. So I don't want people to feel like you have to be in Miami to get these services.
[00:39:51] By all means, please visit our website. We have so many other ways to help people just to get the ball rolling, just to start in the right direction to identify your own neurological sleep disparity. Absolutely. And we chatted about that a little bit earlier, too. And another thing we chatted about that I want to make sure the listeners know, too, is you showed me something really cool earlier. Do you want to mention that? Absolutely. So I'm so excited.
[00:40:15] I actually met this wonderful woman and she is the founder of the Wonder Pillow. Let me see. We actually met an event, a mutual event. I guess I can say it. We met at Shark Tank. I also auditioned for Shark Tank. We are a startup. We are new. We are the first of its kind neuro-restorative sleep center. So I do need support. But from that perspective, I met Betty. She's the founder of the Wonder Pillow.
[00:40:44] We met because at Insomnia Sleep, when our patients don't use a bed, right, they actually sleep upright in a chair because our sleep sessions are only one hour. It's not like the typical go to the hospital, go to a hotel, have the overnight sleep setting. No, our sleep sessions are one hour. Like anyone can come for an assessment. So what she has developed is so wonderful. When people come for an insomnia sleep session, we have this pillow because they're essentially up in a chair.
[00:41:13] We don't want their necks going all over the place. We don't want to keep them upright. And as an anesthesia professional, we are airway specialists. This is what we focus on. And this is why we can use anesthesia to the capacity that we do because we know how to manage an airway. Part of that is we were using these travel pillows. This is in the past. When I met Betty in the Wonder Pillow, her invention allows us to use this for our patients. So all of our patients, they get their own Insomnia Sleep pillow.
[00:41:41] And the beautiful thing about this as well is we use the pillow like this is how the pillow is actually designed, right? And for our sleep apnea patients, a lot of people ask us if you have sleep apnea, can you get a neurorestorative assessment or the therapy? At this time, no. We do not. We're not advocating sleep apnea and anesthesia to be used at the same time. However, we do treat our sleep apnea patients with our sleep apnea program. We are sleep center. We have to help our patients in every capacity.
[00:42:11] For our sleep apnea patients, we do recommend our Wonder Pillow. So with the Wonder Pillow, they will go home. The beautiful thing about the Wonder Pillow, the Wonder Pillow has specifically worked with us at Insomnia to develop a sleep apnea Wonder Pillow. With the sleep apnea Wonder Pillow, it allows the airway to stay elevated and extended, especially for people who have large tongues. It keeps the tongue out of the airway and it does not obstruct the airway like it used to. But this is specifically for Insomnia.
[00:42:40] So we've been working with the Wonder Pillow. I'm so excited. I just wanted to give her a shout out because she's also made, you know, our own brand and our own line of Insomnia Pillows. However, beauty and why she was at Shark Tank and why she's so different is because it is the Wonder Pillow that goes this way with a blanket Layla look. I know that's so awesome. Isn't that so awesome? And our patients get cold, right? Naturally, when you go to sleep in your deep, your body temperature drops. You get cold.
[00:43:10] You're supposed to. We even recommend people make your sleeping environment like a cave. Cold and dark. Cold. The Wonder Pillow already has a blanket attached and it's so great for traveling. We took it for my son's graduation over to Sarasota in the car. It was awesome. So I'm so happy to Betsy and the Wonder Pillow and her success and them working with Insomnia Sleep specifically for our sleep apnea patients and actually all of our sleep patients.
[00:43:39] And I think that's a great travel device. Because even if you don't have sleep apnea, this is such a great travel device. And, you know, this is new. So I'm super excited about Betsy. Please follow her. If not go to our website, we definitely have them. And all of our Insomnia patients get their own Wonder Pillow as well. So, again, thank you so much, Lila, for asking. Of course. No, I think that that's so cool. I've actually seen that online. So it's fun to see that you have that collaboration now. And I've seen it.
[00:44:07] I was like, I need one of those because as someone, whenever I travel, I sleep. So I usually have a pillow or like a hoodie or something. Yes, absolutely. And for me, I like to travel light. So as light as possible. So I always have my carry on. So having that one object instead of having to have a pillow blanket, like nice and concise. It's a really good product. So, yeah. So also, yeah, you know, I'm glad you brought that up, too. If you go to if you order through us, but if you order through Wonder Pillow,
[00:44:33] Wonder Pillow slash Insomnia Sleep, definitely, you know, use our link. You'll get 5% off as well as some other Insomnia goodies. So we definitely welcome the collaboration. That's awesome. It's always so fun to speak with you. I love talking to you. I always learn so much and I always love to learn what you're up to, too, with all your new endeavors and things like that. So that's always that's fun. And that's a very, very cool product. I must say. And I think that also just like to wrap up this episode, one of the key takeaways, I
[00:45:02] think, is that the big shift here is pretty simple when it comes to sleep problems because they're not one size fits all. And I think that now that we know about all these different brain level endotypes with different mechanisms and why that's so many people really are misclassified or misunderstood is because of all these differences. So I think once you really identify the pattern, you stop guessing and you really start targeting the actual cause. So I think that's a huge value of the neuro restorative sleep endotypes framework overall
[00:45:31] and what it really is able to unlock for the future of sleep care, because like we've said before, the goal isn't more sleep. It's restored sleep. So it's a great episode. I think I learned a lot. I love how you broke everything down and I'm sure our listeners definitely learned a lot as well. And for our listeners, make sure that you are following, sharing and subscribing to the show. Nairi, it was great speaking with you as always. And I cannot wait to chat with you soon. I know we have a good episode coming up next month as well. I love it. Yes.
[00:45:59] So again, you know, visit our website insomnia sleep.com. Remember it's insomnia without the I and take our neuro restorative sleep quiz. Let's figure out like what your endotype is. Even if you don't want to come to Miami for your assessment right now, let's get you started. Let's figure out, talk to me, sign up for a consultation, go to our app, get our book Why We Don't Sleep on Amazon definitely explains more, goes in more depth, explains narcolepsy, idiopathic hypersomnia, our silver sleepers.
[00:46:29] What happens neurologically as we get older, you know, with our parents, our grandparents, you know, even you, you may see your sleep schedule start to shift as you get older. We're only company out there looking at sleep from a neurological perspective. We're not sedation, we're restoration. So stay rested my friends. Absolutely. Bye. I'll talk to you soon. Thank you. Bye.